Facial paralysis is a medical condition that affects the movement of muscles in the face, often resulting from injury, infection, or neurological disorders. One of the important considerations in facial paralysis is its impact on muscles related to mastication, or chewing. Understanding which muscles of mastication are affected is crucial for both diagnosis and treatment, as impaired chewing can influence nutrition, oral health, and overall quality of life. This topic explores the relationship between facial paralysis and the muscles of mastication, detailing anatomy, functional consequences, and clinical considerations.
Anatomy of Muscles of Mastication
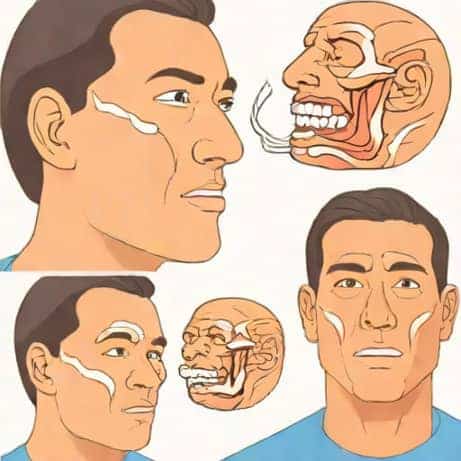
The muscles of mastication are primarily responsible for moving the jaw during chewing, allowing the breakdown of food into smaller ptopics. These muscles are innervated by the mandibular branch of the trigeminal nerve (cranial nerve V3) and include the masseter, temporalis, medial pterygoid, and lateral pterygoid muscles. Each muscle has a specific role in jaw movement, such as elevation, depression, protrusion, and lateral movement. Proper coordination of these muscles is essential for effective mastication and maintaining a healthy oral function.
Major Muscles of Mastication
- MasseterA powerful muscle located at the jaw angle, responsible for elevating the mandible and closing the mouth.
- TemporalisA fan-shaped muscle on the side of the head that elevates and retracts the mandible.
- Medial PterygoidAssists in elevating the mandible and moving it side-to-side.
- Lateral PterygoidHelps in protruding the mandible and enabling side-to-side grinding movements.
Facial Paralysis and Its Impact
Facial paralysis typically affects the muscles innervated by the facial nerve (cranial nerve VII). These muscles control facial expression, including movements of the lips, cheeks, and eyelids. However, the muscles of mastication are innervated by the trigeminal nerve, which is distinct from the facial nerve. This anatomical distinction has important implications for understanding which aspects of chewing are affected by facial paralysis.
Which Muscles Are Affected?
Since the muscles of mastication are supplied by the trigeminal nerve, facial paralysis does not directly paralyze these muscles. Therefore, the masseter, temporalis, medial pterygoid, and lateral pterygoid remain functional. This means that jaw elevation, depression, and lateral movements can still occur, allowing a person with isolated facial paralysis to chew food mechanically. However, facial paralysis indirectly affects mastication by impairing the muscles of facial expression, which support oral function during chewing.
Indirect Effects on Mastication
Even though the muscles of mastication remain intact, facial paralysis can interfere with the efficiency of chewing. The orbicularis oris and buccinator muscles, which are innervated by the facial nerve, play a critical role in controlling food within the oral cavity. These muscles help keep food positioned between the teeth and prevent it from spilling into the cheeks or lips during chewing. When facial paralysis weakens these muscles, patients may experience difficulty in handling food properly, leading to inefficient mastication and increased risk of choking or drooling.
Specific Muscles Involved in Oral Support
- Orbicularis OrisEncircles the mouth and helps seal the lips to prevent food from escaping during chewing.
- BuccinatorForms the muscular wall of the cheek, keeping food between the teeth for effective grinding.
- Risorius and Other Facial MusclesAssist in lateral movements of the cheeks and maintaining oral symmetry, indirectly aiding mastication.
Clinical Implications
Understanding the indirect effects of facial paralysis on mastication is important for clinical management. Patients with facial paralysis may require interventions to improve oral control and maintain effective chewing. This can include physical therapy, exercises to strengthen the orbicularis oris and buccinator, and dietary modifications to ensure safe swallowing. Additionally, dental care may be necessary to prevent complications such as tooth wear, gum injury, or aspiration of food due to reduced oral control.
Rehabilitation Strategies
- Facial Muscle ExercisesTargeted exercises can help improve strength and coordination of facial muscles involved in oral support.
- Speech and Swallowing TherapySpeech-language pathologists can provide guidance on techniques to safely chew and swallow food.
- Dietary AdjustmentsSoft or chopped foods may be recommended to reduce strain on weakened oral muscles.
- Assistive DevicesIn some cases, specialized dental devices or oral aids can help keep food properly positioned during mastication.
Summary of Effects
In summary, facial paralysis does not directly affect the primary muscles of mastication such as the masseter, temporalis, medial pterygoid, or lateral pterygoid. These muscles remain functional because they are innervated by the trigeminal nerve. However, facial paralysis affects muscles of facial expression, including the orbicularis oris and buccinator, which indirectly influence mastication by controlling food placement in the mouth. The result can be inefficient chewing, spillage of food, and potential challenges in swallowing, highlighting the importance of a comprehensive clinical approach to care and rehabilitation.
Facial paralysis primarily affects muscles involved in facial expression, not the muscles of mastication directly. However, the orbicularis oris, buccinator, and other supporting facial muscles play a crucial role in managing food within the mouth during chewing. When these muscles are weakened due to facial paralysis, patients may experience difficulty in handling food efficiently, which can impact nutrition and overall oral function. Effective management involves understanding the indirect effects on mastication, implementing therapeutic exercises, and providing appropriate dietary modifications to ensure safe and effective chewing. By addressing both the direct and indirect impacts of facial paralysis, patients can maintain oral health and improve quality of life despite the challenges of this condition.